Book: Introduction
| Сайт: | Dementia Family Carer E-Learning Courses |
| Курса: | Later Stage Dementia Care - Blended Learning for Families (Final Template) |
| Кніга: | Book: Introduction |
| Надрукавана: | Invitado |
| Дата: | панядзелак, 9 чэрвеня 2025, 1:24 AM |
1. What is later stage dementia?
The fact that dementia is a progressive, incurable and life limiting disease is not always raised.
Dementia is not one specific disease. Rather dementia describes a collection of symptoms that are caused by disorders affecting the brain.
Dementia affects thinking, behaviour and the ability to perform everyday tasks. Brain function is affected enough to interfere with the person’s normal social or working life.
Hanson (2019) has written that "The progression of dementia is often separated into mild, moderate and severe corresponding to early, mid and late or advanced stages. The middle to late stages of the disease often signals a loss of autonomy, independence and reduction in physical and cognitive function."
Therefore, a person in the later stages is likely to experience severe memory loss, problems with communication and daily activities, and greater changes in behaviour and physical problems than in the earlier stages. They will probably rely on others for much of their care.
In this course we will use the term 'later stage dementia' to describe people who have had dementia for some years. The term 'end of life’ stage will be used to describe the last months and weeks, days and hours of the person with dementia, just before death.
2. Learning Goals
This week we will look at some of
the terminology and definitions used in later stage dementia care. This is for
your information generally, but it will also help you as the course progresses.
We will also examine how to recognise when the person you are caring for is in the later stages of their dementia. As we will see, sometimes there are difficulties involved in recognising differences in the stages in dementia.
3. Person-centred care
Before we start looking at the
Later Stages of Dementia Care in detail, we need to look at our Philosophy of
Care
What do we mean by Care? What is our attitude to caring, and to a person who needs care?
In The Alzheimer Society of Ireland we believe in 'Person Centred Care'. Person centred care is a concept that recognises the needs and perspectives of the person with dementia as being important.
“Person-centredness is an approach to practice established through the formation and fostering of healthful relationships between all care providers, service users and others significant to them in their lives. It is underpinned by values of respect for persons (personhood), individual right to self determination, mutual respect and understanding. It is enabled by cultures of empowerment that foster continuous approaches to practice development” Mc Cormack & McCance (2016).
Here are two links to help you explore notions of person-centred care.
HSE: Person and Family Enagement
Person centeredness is about everybody and for everybody.
It is about understanding each other.
It is about respecting each other. Here is a link to the This is Me booklet produced by The Alzheimer Society UK. It allows you to record and document some of the characteristics and personality of the person you are caring for. This can be very useful if he or she needs to go to a Day Care Centre, hospital or to another place where your loved one is not known.
It is about recognising each other.
It is about a sharing and coming together.
4. Personhood in dementia
Personhood is another part of our Philosophy of Care in The Alzheimer Society of Ireland.
Personhood is a concept that is given to us by others in our society and in our relations e.g. we are ‘a father, a wife, a boss, a Reader at Mass, someone who walks her dog every day.’
Tom Kitwood (2007) defines personhood as “A status or standing bestowed on others” .
McCormack (2016) expands and says that there are 4 elements to Personhood
- Being in a social world: persons are social beings
- Being in Relation to others: persons exist in relationships with other persons
- Being in Place: persons have a context through which their personhood is articulated
- Being with Self: being recognised, respected and treated as a person impacts on a person’s sense of self.
5. Later stage dementia - stage 3
In this third and final stage,
the person has severe impairment and needs total, 24 hour care. The person may:
· Lose their ability to understand or use speech
· Need help with eating, washing, bathing, toileting and dressing (these are sometimes called the Activities of Daily Living)
· Be disturbed at night
· Be restless
· Show little or no recognition of family and friends
· Have difficulty walking, eventually perhaps becoming confined to a chair
· Have permanent immobility, and in the final weeks or months the person will be bedridden.
· Be incontinent
It’s important to remember that some abilities remain throughout all stages. The person still keeps their sense of touch and hearing, smell and their ability to respond to emotion.
A person in the later stages of dementia may have symptoms that suggest that they are close to death, but actually live with these symptoms for many months.
6. Palliative care
Palliative care is defined by The
World Health Organisation as 'an approach to care that improves the quality of
life of patients and their families facing problems associated with
life-threatening illnesses, through the prevention and relief of suffering by
means of early identification and impeccable assessment and treatment of pain
and other problems including physical, psychosocial and spiritual' (WHO 2001).
Psychosocial means the mixture or combination of psychological and social. For people living with dementia this may mean factors such as loss of autonomy, grief, fear, loneliness and financial constraints. It may mean stress, anxiety, depression, social isolation, and poor relationships
The aim of palliative care is to enhance quality of life. Palliative care also extends support to families to help them cope with their family member’s illness and their own experience of grief and loss.
So, palliative care is the holistic care of people with a life-limiting illness that seeks to maintain quality of life and to relieve suffering for the person with the illness and their family.
This will be discussed more in Units 2, 4, 5 and 6.
7. Principles of palliative care
There are a number of important principles associated with palliative care. These include the following:- Affirms life and regards death as a normal process
- Neither hastens or postpones death
- Provides care that is person-centred and focused on the whole person
- Provides relief from pain and other distressing symptoms
- Offers a support system to help individuals live as actively as possible until death
- Promotes quality of life and choice for the individual and family
- Offers a support system to help families cope during the person’s illness and during their own bereavement
- Values and promotes interdisciplinary team-working

8. Conceptualizing Later Stage Care
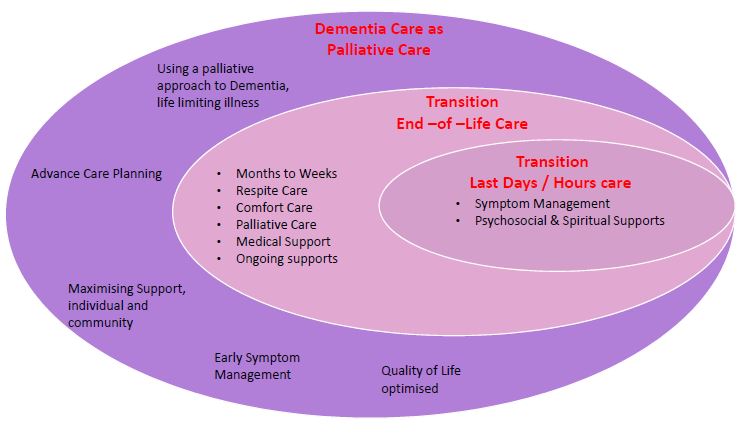
Source: Interior Health, Canada. More information at: https://www.interiorhealth.ca/YourCare/PalliativeCare/Pages/WhatIsPalliative.aspx
Dementia Care as Palliative
Care - A Palliative Care approach optimises quality of life and can ease
the journey for both the person with dementia and their families. This approach
includes treating and managing early symptoms and behaviours in collaboration
with available Healthcare and Voluntary Supports Groups, and may also include
input from a Hospice Team. Advance Care Planning can help ensure that the
person’s wishes and preferences are considered and that they die with dignity. More
details in Unit 2, 4, 5 and 6.
Transition – End of Life Care - People with dementia may be in the end stage of their illness for many, many months. The goals are to support living well to the end of life – a continuum rather than a point in time. Care may be guided by the person's known wishes and individual choices are respected. Providing emotional support for the person’s family and friends is important. More details in Unit 2.
Transition – Last Days and Hours Care - The last days and hours is the time when the person is still alive bit time is short. It is a time for being with rather than doing for. It is the time to provide care for pain (if needed) and other symptoms. It is the time to look at spiritual and emotional needs of the person and the family /friends. More detail in Week 2.
9. Case Study Exercise
What are case studies?
We will be using a Case Study as a teaching and learning aid on this course. Each week we will outline a scenario as it relates to each Unit. We will ask you to consider some questions for discussion and debate.
We will be looking at the life of Tony, a man living with dementia. The Tony Case Study is not a real case study. Any references to real people, names, characters, places, and incidents and any resemblance to persons, living or dead, is entirely coincidental. The details described each week are for educational purposes only.
There are no right or wrong answers necessarily to questions posed in the case studies.This Week's Case Study
This week we would like to introduce you to Tony.
Tony is a retired business man who lives in the midlands with his wife Maura. They are both in their 70’s and have been married for nearly 50 years. They have 1 son who lives abroad, and whose job takes him to remote parts of the world for many weeks at a time.
Tony was a shopkeeper (in a different larger town) for many years. They moved to this town 5 years ago and enjoy the gentle pace of living in a small community. They have neighbours and friends but generally like their privacy. Tony used to play golf less so now, used to travel less so now, and they both like to tend to the garden, though it has been neglected of late.
Approximately 7 years ago, Tony was having trouble with his memory and other symptoms and was diagnosed with Alzheimer’s disease.
Over the past years, Tony has needed more help in every way. His mobility is compromised, he needs help getting dressed and is sometimes incontinent. Tony sometimes gets lost on his way to and from the local shop. Sometimes Tony has difficulty saying what he wants to, and sometimes he doesn't seem to be listening. Tony gets help from the HSE in that a lady (Home Care) comes every morning for 30 minutes to help him get up etc. There is a lot of change of staff and Tony never knows who is coming. Tony goes to a dementia specific day center 3 days per week and he enjoys this as he spent most of his life working as a shopkeeper and meeting people daily.
Maura’s overall health is good, she likes driving and likes to cook and bake. Sometimes Maura gets anxious thinking about the future and what it will bring.
Consider the following:
1. Where do you think Tony is on his dementia journey?
2. What do you think of his daily routine? Would you consider it to be person-centred?
3. What changes, if any, would you consider if you were Maura?
Having read about Tony and Maura, you can discuss their situation and the questions above on the Forum: Unit 1 Case Study