Book: End of Life Symptoms
| Site: | Dementia Family Carer E-Learning Courses |
| Course: | Later Stage Dementia Care - Blended Learning for Families (Final Template) |
| Book: | Book: End of Life Symptoms |
| Printed by: | Гість-користувач |
| Date: | Sunday, 8 June 2025, 4:55 PM |
1. End of Life stage
When the person with dementia moves to the end of life stage, their symptoms too will change. This book outlines some of these physical changes and sets out measures you can take to support your loved one at this time. Emotional changes for the person with dementia will be discussed in Unit 4 Emotional Well-Being for the Person with Dementia, and for the Carer in Unit 5 Coping and Self-Care.
2. Learning Goals
Learning Goals
By the end of this unit we hope you will have a clearer understanding of the likely symptoms that a person with dementia will experience in the end of life stage.
3. What are the signs of end of life stage?
It is difficult to know when a person with dementia is coming to the end of their life. However, there are some symptoms that may indicate the person is at the end of their life including:
-
limited speech (single words or phrases)
-
needing 24 hour help with everyday activities
-
eating less and swallowing difficulties
-
incontinence and becoming bed bound.
When these are combined with frailty, recurrent infections and/or pressure ulcers, the person is likely to be nearing the end of their life. If the person has another life limiting condition (e.g. cancer), their condition is likely to worsen in a more predictable way.
When a person gets to within a few weeks, days or hours of dying, further changes are common. These may include:
-
deteriorating more quickly
-
loss of consciousness
-
inability to swallow
-
becoming agitated or restless
-
irregular breathing
-
cold hands and feet.
Often, the last hours of life are the time when some family members most want to communicate with their loved one. Some family members may find this stage distressing. It may be helpful to surround the person with the people, things, music, and sounds that he or she would like and include the person in everyday conversations. It may be the time for family members to say the things they need to say.
4. Prioritizing care goals
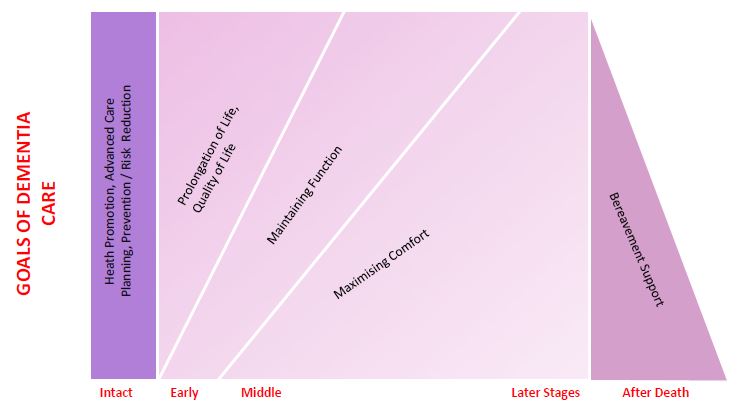
This is another diagram that represents dementia care.
This diagram shows dementia care goals and priorities throughout the course of dementia. It shows that in Early/ Middle stage dementia Quality of Life is the priority but in Later Stage ‘Maximising Comfort ‘is the main goal.
These are also the goals identified by Palliative Care that we talked about in Unit 1
These goals of care include a Person-centred care approach, which recognises the needs and perspectives of the person with dementia as being most important. We have explored this already in the Book: Introduction, page 3 on Person-centred care.5. Pain
A person may still feel pain in the later stages of dementia even though
they may not be able to verbally communicate it. It’s important to consider
pain as a cause of unusual behaviour and make sure that it is properly managed.
Many people in the later stages aren’t given enough pain medication and may be left in pain that could otherwise be treated.
Common causes of pain in people with dementia include urinary tract and other infections, constipation and other conditions (for example arthritis). If you think the person may be in pain, speak to a GP about medication. Also consider non drug approaches (such as change in position, movement or massage) that may help relieve the pain, albeit temporarily.
6. Delirium
Delirium can occur in all stages of dementia and can be very distressing for the person with dementia and their families. Delirium may be present at end of life.
How do I know if the person with dementia has delirium?
Delirium usually begins suddenly. The person may seem unaware of what is going on around them and be confused and inattentive. Their level of consciousness can vary and the symptoms can fluctuate. Other signs and symptoms include:
-
ACUTE restlessness and agitation
-
drowsiness and slow responses
-
hallucinations
-
disturbed sleep
-
emotional changes, such as fear and anxiety.
6.1. Causes of delirium
There are many possible causes of delirium and there is often more than one cause.
The most common causes include
- infections; often kidney/ urine infections or chest infections
- dehydration, constipation, urinary retention (not passing urine) and/ or pain
- low oxygen levels including breathlessness and fatigue
- Electrolyte disturbance (high or low sodium, usually dehydration), glucose (diabetes), calcium (caused by medications or medical condition). ‘Bloods’ need to be checked
- Kidney ( renal) or liver impairment
- medications, such as opioid (morphine based) painkillers, steroids and antidepressants
- withdrawal from drugs, including alcohol, sedatives and antidepressants
Depending on the cause, delirium can often be reversible. It is therefore important to contact medical services (see next page).
However, delirium that develops in the last few hours and days of life may not be reversible.
6.2. Delirium and agitation
Agitation may be present for some people throughout all stages of dementia. (Unit 2)
Agitation may be a symptom of delirium.
And in the last months or weeks or days, agitation might be due to symptoms such as breathlessness or pain. The person might fidget and be unable to settle. They might be picking or grabbing at bed clothes, moaning and calling out.
Agitation, like delirium can be frightening for the person and distressing for family and friends.
It’s important to talk with Professionals about what could be causing it, and what might happen next.
6.3. Delirium - how can I help?
If you see a change in the person’s mental state or if you’re concerned
about safety, then you should contact the GP, Public Health Nurse or specialist
nurse.
Also consider the following:
· Keep the environment calm and quiet, and if you can, limit the number of visitors. Try to keep the person in a normal sleep-wake pattern by using lights at the appropriate times, and reducing noise and stimulation at night.
· If you think that delirium may be caused by withdrawal from nicotine, then nicotine replacement therapy, such as patches, may help to reduce symptoms.
· Help the person to drink and eat regularly
· Do not move the person unnecessarily
The Doctor may consider investigations and treatments, where appropriate, of underlying and reversible causes of delirium, such as infection, dehydration and electrolyte imbalance.
Doctors may try a low dose of a sedative or an antipsychotic. (Doctors won’t give an antipsychotic to a patient with Lewy body dementia, because of the risk of side effects.)
The role of medication in delirium at end of life is controversial. Drugs do not replace good nursing and supportive care.7. Food and hydration
In the end stages of dementia (that is, in the last few months or weeks
of life), the person’s food and fluid intake tends to decrease slowly over
time. The body adjusts to this slowing down process and the reduced intake. It
is thought that in Later Stage the hunger and thirst part of the brain (hypothalamus)
has now stopped functioning for most people.
The person may be immobile and so not need the same amount of calories to sustain their energy levels. Having reduced food and fluid intake and decreased interest can be thought of as a ‘natural part’ of end of life and dying.
As dementia progresses it affects the area of the brain that controls swallowing. In advanced dementia the person may have a weak swallow or lose the ability to swallow safely.
7.1. Is the person suffering?
Whether or not a person living with later stage dementia is suffering is a most common concern for Carers. Carers are often unaware of why the person is having difficulty swallowing or does not want to eat or drink anymore.
The PHN or GP can help explain why this is happening: as a person with advanced dementia takes less and less food and fluid towards the end of life and their body adjusts so that they do not feel hungry or thirsty. The hunger and thirst part of the brain has now stopped functioning for most people.
Therefore, people are not suffering.
Providing comfort care is important and mouthcare can be soothing for the person
In people who are conscious, the mouth can be moistened every 30 minutes with water from a water spray or dropper or ice chips can be placed in the mouth. In unconscious people, moisten the mouth frequently, when possible, with water from a water spray, dropper, or sponge stick or ice chips placed in the mouth. To prevent cracking of the lips, a water-soluble lubricant should be applied.
If there are signs of pain or discomfort, seek the advice from the Public Health Nurse or GP.
7.2. Artificial nutrition and hydration
Artificial nutrition and hydration is the giving of fluids and nutrition
via an intravenous cannula (IV) or an enteral tube, for examples PEG tubes.
Research informs us that artificial nutrition and hydration does not alter the outcomes for the person with dementia. It should not be considered for someone with end stage dementia where swallowing difficulties are a feature.
Using artificial nutrition and hydration poses many ethical and practical dilemmas for people with later stage dementia.
Consultants and GP’s have knowledge and expert experience in this area. Discussing your concerns may help.8. Other symptoms at end of life
Difficulty breathing
People with dementia at the end of life care stage may have difficulties breathing. If this is a new symptom or you feel it is causing your loved one distress ask for a medical review. They may change the position of the person in the bed, or may give medication which may relieve some of the distress.
Nausea/vomiting
Nausea or vomiting may occur for the person at the end of life care stage. Medications to reduce the symptoms can be given orally/as an injection.
Constipation
If the person has not had a bowel motion in a number of days, they may or may not be constipated. Discuss your concerns with the medical health care team.
Anorexia / Weight Loss
Anorexia and weight loss can be a normal part of the end of life stage of care. The body is winding down and does not require as many calories. The sense of hunger is also reduced for the person with dementia at this stage. If you are concerned speak to a health care professional.
Fatigue
As part of the winding down of the body in the end of life stage the person may become very fatigued and spend a lot of time sleeping.
Anxiety and Depression
If you feel your loved one is showing signs of anxiety or depression talk with your doctor or someone else on your care team about them. Get immediate medical help if you or a loved one is having thoughts of suicide.
Fever
Fever and sweating are common in the last days of life. This may be caused by infections, medications or other medical conditions. If you notice this inform the health care team.
Comfort care is a priority at this stage and the health care team can help e.g. environmental changes, such as a fan in the room or lighter blankets or removing direct sunlight on to the bed by adjusting the blinds.